What's been considered America's 'gold standard' of autism therapy may not work — and those who have been through it are pushing back

Jerry Holt // Star Tribune via Getty Images
What’s been considered America’s ‘gold standard’ of autism therapy may not work — and those who have been through it are pushing back
a young boy takes some time away from ABA therapy to play a game on family computer
In 1987, a prominent University of California, Los Angeles psychologist published the culmination of his life’s work — and spurred headlines across the globe. Ole Ivar Lovaas claimed that delivering a new therapy one-on-one for 40 hours a week had made nine of 19 autistic children “indistinguishable from their typically developing peers.” Half his subjects, he reported, saw 30-point IQ gains, learned to speak normally and were able to function alongside other students.
It was huge news. At the time, an autism diagnosis frequently meant life in an institution for the child in question. The opening of a path to a version of a “normal” life seemed nothing short of a miracle. Few people questioned the history of Lovaas’ research or the ethics of his methods.
Rather, determined to do right by their children, parents fought hard to get the new therapy, dubbed applied behavior analysis, or ABA — though it was as expensive as it was supposedly game-changing. Today, there is an excellent chance that a child diagnosed as autistic will receive a referral to a provider of ABA, routinely described as “gold standard” therapy that uses behavior modification techniques to eliminate traits deemed undesirable.
The 74 reports that as the rate of U.S. children identified as autistic has risen to 1 in 36, an entire industry has grown up around them. Where once parents had to sue to force school systems, social service agencies and insurers to pay for what was billed as an autistic child’s only fighting chance, today there are ABA treatment centers where families and schools can send a child; therapist degree programs; at least 100 companies running networks of ABA centers; countless stand-alone programs; dedicated ABA schools that students attend full time at public expense; and ABA training for special education teachers. With all this comes the potential for profit — up to $2.45 billion a year, according to investment firms — and thus an army of lobbyists and public relations specialists making sure ABA is the first, and often only, therapy available. Armed with testimonials of success, parents became — and many remain — their zealous ambassadors.
(Mac Dawson, pictured above, takes a break from his ABA therapy, which he has done for 36 hours a week for the past four years)
The pushback against ABA begins
But 37 years after Lovaas’ bombshell article, researchers, therapists and autistic adults who themselves were ABA patients as children are pushing back. Proponents of other approaches and some educators — as well as the U.S. Education Department — have expressed frustration over the depth with which ABA has become ingrained, to the exclusion of other therapies and the potential detriment of potentially hundreds of thousands of children. A critical mass of advocates is challenging the notion that non-disabled diagnosticians should get to decide how autistic children should be treated — indeed, how the entire concept of disability should be defined.
The U.S. Department of Defense, among other research organizations, has called into question whether ABA actually works. And scholars are investigating whether it causes harm to the children subjected to it. Some who experienced the intervention say it absolutely does.
The problems with ABA started early on, beginning with Lovaas’ own beliefs.
“You start pretty much from scratch when you work with an autistic person,” he told Psychology Today in 1974. “You have a person in the physical sense — they have hair, a nose, a mouth — but they are not people in the psychological sense.”
This lack of humanity, Lovaas did not shy away from saying, justified using electric shocks, slaps, withholding of food and other forms of physical punishment to “extinguish” autistic traits — even joyful ones — and replace them with “normal” behaviors.
Simultaneously, Lovaas was using the same methods to “treat” suspected homosexuals and transgender people — so-called conversion therapy, which was quickly recognized as a human rights abuse. But the same reasoning that propelled the research community to turn away from using “operant conditioning” on LGBTQ people was not extended to autistic children. Instead, proponents charged ahead — even though Lovaas’ own landmark study does not come close to what many current researchers deem credible.
The Norwegian-born psychologist, who died in 2010 at age 83, had personally decided which children received his pioneering intervention and which became the control group. Six years after his initial publication, Lovaas conceded that ABA becomes less effective over time, because, “These people are so used to pain that they can adapt to almost any kind of aversive you give them.”
More concerning, a growing body of research from, among other sources, the U.S. Department of Defense and a multi-disciplinary team of university scholars called Project AIM has found the evidence base for ABA is too thin and of too poor quality to justify its widespread adoption. The majority of studies that have found it effective are rife with industry conflicts of interest.
And many former patients who were subjected to ABA as children believe the treatment is abusive. One 2018 survey found that just 5% of autists — a term used by some people with autism — support the therapy, with a majority of neurotypical relatives of autistic people opposing it.
As neurodivergent adults have moved into the ranks of academic and independent researchers, some have begun compiling evidence that ABA subjects are more likely than other autists to suffer from PTSD and other serious mental health problems.
“It doesn’t seem to be on anyone’s radar that these interventions could cause harm,” says Kristen Bottema-Beutel, a Boston College professor and an author of the Project AIM meta-analysis. “There seems to be this unwillingness to listen to autistic people who say that it does.”
It’s a Catch-22, she continues: “There’s no evidence. But the reason there’s no evidence is because we are unwilling to collect it.”
![]()
The 74
‘My monkey tricks were impressive but dehumanizing’
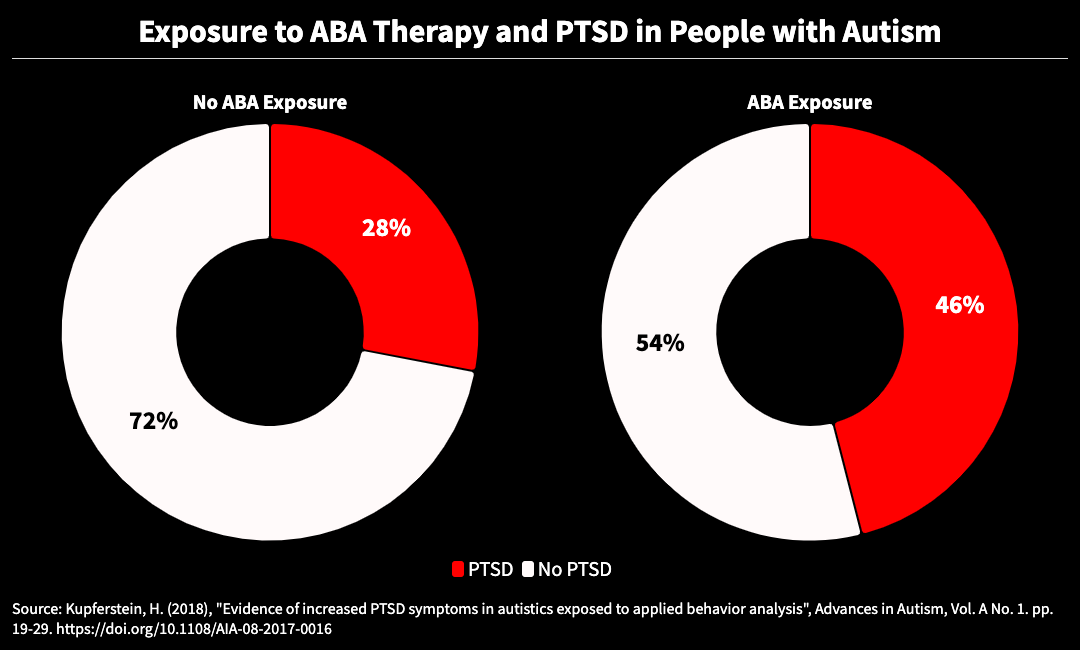
two donut charts showing Exposure to ABA Therapy and PTSD in People with Autism
Unlike Lovaas, most of today’s ABA therapists don’t wield paddles or electric shocks. But they continue to push for compliance in ways many parents and autistic adults describe as controlling and abusive. There’s no more slapping, but toys, treats and — possibly most damaging — attention are frequently withheld when a child is not compliant. The goal remains “extinction” — the term still used for the process of drilling until an autistic behavior no longer takes place. The centerpiece of this conditioning still bears the name Lovaas gave it: the discrete trial.
Often delivered for long periods, and beginning at ages when children are too young to sit still and obey commands, ABA involves a therapist giving an instruction — such as asking the child to make eye contact, fold their hands in their lap or speak out loud. Positive and negative feedback comes repeatedly and rapid-fire, sometimes including physical reinforcement like turning the child’s head or holding their hands down. When the patient complies, a new command is introduced.
Sometimes, the targeted behavior is dangerous for the child, such as head-banging, or exhausting for caregivers, such as smearing food or feces. Other times, it’s simply a visible deviation from “normal.” Either way, the goal is to train the child to respond differently to the surrounding environment.
The upshot, say many adult autists, is that because patients appear more neurotypical, non-disabled people may believe they are “better,” when in fact they may well have sunk into a state of burnout and are developing mental health issues.
From a non-autistic perspective, many of ABA’s goals seem entirely reasonable — indeed, even a kindness undertaken to facilitate a child’s chances of social acceptance. It’s hard to make neurotypical friends, the reasoning goes, if your affect is flat or you make guttural noises when you are excited. Teachers can’t deliver lessons if they’re trying to keep a student from bolting from the classroom. It’s nigh unto impossible for a parent to finish the grocery shopping with a kid who has melted down and may be physically out of control.
ABA, autistic adults say, may train a child to stop some of these behaviors. But it does nothing to address the underlying causes or teach coping skills, and comes at a tremendous psychological cost. To someone who is easily overstimulated, buzzing fluorescent lights, hyperactive siblings, or continual changes of setting and activity can make classrooms and public spaces a sensory nightmare.
Take, for example, the common ABA goal of asking a child to make eye contact. While there are several levels of expertise, and therapists’ training varies, the board that certifies ABA practitioners “requires no education and training on autism in general, let alone [its] cognitive and neurological characteristics,” the journal Cogent Psychology reported in 2019. So therapists who compel eye contact — even going so far as to turn the child’s head so they are face to face — may not know that it overstimulates the portion of autistic children’s brains that is primarily responsible for anxiety.
One way autists cope with anxiety is to “stim” — make sounds or movements, such as hand-flapping or rocking, that discharge this overstimulation. The more overstimulated a child gets, the more pronounced the behavior. Unable to self-soothe or leave an overwhelming environment, the child is likely to melt down. In trying to eliminate stims, the authors of the Cogent Psychology article report, ABA makes “arbitrary distinctions between which movements are pathological and which are not.”
“A lifetime of being punished for certain movements, and being forced to engage in eye contact despite the physiological pain and discomfort of doing so, is psychological and physical abuse,” they write. “A lifetime of being forced to sit still with no regard for actual cognitive abilities can create further emotional and psychological harm.”
Autists describe attempting to appear “normal” as masking or camouflaging. It often takes so much effort that it can suck up all of a person’s energy, meaning they may not actually hear a lesson being delivered or be able to engage with a conversation. If directed to do something that is a physical impossibility, a child may not even be able to mask.
Nor will behavioral therapies do anything to change what a person’s neurotype — the scientific label for a brain and body that operate differently — physically prevents them from doing.
“They are neurological problems, not problems with my social understanding or intellect,” one adult who experienced ABA told researcher Laura Anderson for a 2022 report published in the journal Autism.
Research on the harms of masking is mounting. A 2018 study published in Advances in Autism found ABA participants were 86% more likely to meet the diagnostic criteria for PTSD than autistic people who were not exposed to the therapy. Nearly half of those affected displayed PTSD symptoms that would be considered at “extreme levels of severity.”
An emerging body of research suggests that separate from mental health conditions, camouflaging is associated with heightened risk of suicidality, already much greater for autists than the general population.
Summarized one participant quoted in Anderson’s report: “My monkey tricks were impressive but dehumanizing.”
Who wouldn’t want to hear, ‘I love you’?
When Elizabeth’s daughter Lily was diagnosed with autism at age 3, she was told to start ABA as soon as possible, preferably for 40 hours a week. “It’s just overwhelming,” Elizabeth recalls. “I didn’t know anything about the diagnosis. I didn’t understand what it could mean.” (To protect the child’s privacy, Elizabeth and Lily are pseudonyms for a mother and daughter who live in a Massachusetts city that is home to a number of universities.)
A scientist, Elizabeth downloaded all the research she could find and immediately became concerned. Because of ABA’s focus on how many correct responses a child provides, there was data galore. But it documented the number of times it takes to extinguish or create a behavior. None of it told her how Lily’s life might change.
Lily is hyperlexic, meaning that for such a little girl she had a huge vocabulary. But she is sometimes nonverbal. For some autists, speaking out loud may be physically difficult, even impossible. Coordinating the complex physical and mental functions that go into talking may take so much effort that it wears them out or sends them into a meltdown.
A common criticism from autistic adults who experienced ABA is that they used precious energy struggling to say what the therapist wanted to hear just to get the exercise to stop. A therapist may eventually succeed in getting children to name the toy they want, but it often stymies meaningful communication.
Unaware of the hurdles speech can pose, parents are often thrilled when ABA teaches their child to speak — after all, who wouldn’t want to hear, “I love you”? They rarely realize that other approaches could facilitate more interaction while taxing their child less.
In fact, because ABA is frequently offered in place of speech-language therapy or assistive technology — such as programmable electronic “talkers” that allow children to piece together pictures or symbols into sentences or even stories — parents and teachers may not be aware of how much language a child actually has.
Lily spoke as a small child, but as she got older, she would stop talking for a day or two at a time. Elizabeth wanted to teach her to sign but was discouraged by health care providers who had heard from ABA therapists that children given alternate means of communication are less likely to become verbal.
When Elizabeth was first looking into ABA’s research base, she saw that among the evidence that it works was data on the number of times a patient speaks. To her, this was a poor substitute for knowing whether Lily could describe how she felt or what she was thinking about.
Lily now has a device she can use when she can’t or doesn’t want to speak. Often, Elizabeth says, the girl is much more expressive with it.
“You can train any mammal to do the things that ABA can train your kids to do,” Elizabeth says. “How a kid is feeling and growing in terms of their relationships and their anxiety and feeling comfortable with people — that’s really different than sitting at a table and pointing at a picture nine times out of 10.”
Adverse events data should be included in standard in autism research
Based on data gleaned from the nearly 10 million military dependents it insures, the U.S. Department of Defense has repeatedly called the evidence supporting ABA “weak,” noting there is no research to determine whether the small number of participants who show improvement — 15% — do so because of treatment or simply because a child has matured. After a year of the therapy, the department reported to Congress in 2019, 76% of 16,000 participating autistic children saw no change, and 9% worsened.
(The private nonprofit National Academies of Sciences, Engineering and Medicine is conducting a federally mandated review of the Defense Department’s autism intervention research. Its findings are slated for release in summer 2025.)
Even accepting more typical behavior and communication as legitimate goals, research has found scant evidence that the treatment achieves those outcomes. Results of a randomized trial in England, for instance, “suggest lack of clinical effectiveness,” researchers concluded in 2020. A 2010 review of the “Lovaas Method” by the U.S. Department of Education’s What Works Clearinghouse looked at 58 studies, concluding that only two even partially met its standards.
Project AIM’s meta-analysis, published in 2020, found little high-quality research — and little evidence in the investigations that did meet rigorous standards — that supported ABA’s efficacy. Of the 150 investigations undertaken between 1970 and 2018 the Project AIM team examined, 70% had serious conflicts of interest, which less than 6% disclosed.
After an autistic researcher, Michelle Dawson, pointed out that Project AIM had not considered whether the studies it analyzed reported side effects or harm, members reexamined them and found that only 11 included even cursory mentions of participants’ psychological or physical distress.
Including adverse events data should be standard, says Bottema-Beutel, the Boston College professor and Project AIM author: “It is in other fields, and it absolutely isn’t in autism research. … It’s especially important because there is an enormous community of autistic people who say that they have been harmed by participating in these interventions.”
A related flaw in the overall body of research, Bottema-Beutel adds, is that it disregards what autistic people say they want in the way of therapeutic support. “It would be difficult to find studies that were well designed, that don’t have risks of bias [and] that show improvement on meaningful outcomes that autistic people care about,” she says. “Show me an ABA study where they improve quality of life.”
‘It was so humiliating being there’
Concerned about the way ABA-affiliated researchers defined and quantified success, Elizabeth went back to the internet and searched for opinions from autistic adults. “I just wanted to hear from older autistic people who experienced therapy,” she says. “And try to understand that from my daughter’s perspective, because at the time, she certainly couldn’t tell me.”
What she heard were responses like these:
“It resulted in corrosive damage to self-esteem and deep shame about who I really am,” a former patient told a University of California researcher in 2017. “No effort was made to explain autism to me or to explain the role of sensory overload in issues like meltdowns, shutdowns, etc.”
Therapists, another former participant told researchers at the Autistic Self Advocacy Network, “teach you to anticipate that when you say ‘no,’ they’ll bulldoze through that because you don’t own your own body.”
Another said she was left with crippling social anxiety: “All of those things that I was doing wrong would automatically go through my head any time I was in a social situation. … I would be inherently super judgmental and self-critical about everything I was doing to the point where even in some social situations, I just shut down.”
And: “It was so humiliating being there.”
Perhaps the most painful element of the swelling controversy about ABA is the clash of perspectives of neurotypical parents and autistic adults who say — often bluntly — that the effort families are making to do right by their child is misguided. The conversation is especially freighted because both groups have unhappy histories. Until Lovaas, poor parenting was blamed as the root cause of autism. For their part, many autistic adults are enraged that they are not routinely invited to help shape research and policy.
Autistic adults who believe they were harmed by ABA are quick to say they believe their parents were doing the best they could with the information and resources they had. “I am not mad at them for their effort,” one autistic woman told researchers looking into trauma rates. “They weren’t disrespectful. They just had a flawed paradigm for autism, and therefore, what they tried didn’t work. That doesn’t make them bad people.”
ABA does have its advocates
Many parents wholeheartedly believe ABA delivers great victories. Often, they are proud that after their struggles to find services and pay for them, their child talks, follows directions and has far fewer disruptive behaviors.
One of the most visible advocacy organizations, Autism Speaks has played a leading role in helping families of autistic children press for expanded access to ABA and other services.
The organization’s stance on ABA is that it may be effective for some people and not others; therapies should be tailored to the individual and should not attempt to enforce behaviors based on social norms. When implemented properly, the organization holds, “ABA can lead to improvements in IQ, adaptive behavior, communication skills, social skills and a reduction in challenging behaviors.”
The evidence behind behavioral science is sound, says Andy Shih, Autism Speaks’ chief science officer. But as with any other treatment, there can be differences in how a therapy is conducted — particularly given the range of training and experience among therapists. A skilled practitioner working in the right conditions can succeed in changing behavior, he says, most notably eliminating those that endanger a child.
“Everybody experiences ABA differently,” says Shih. “The setting in which we see them, the quality of the service provider, they all make a difference, I think. In general, even though there are established standards and criteria in terms of what a good autism service should look like … just like in other branches of medicine, what is ideal and what is actually delivered, sometimes there’s a big gap.”
Eileen Lamb, director of social media for Autism Speaks, credits nine years of ABA for helping one of her children, who is nonverbal and has a potentially dangerous eating disorder called pica. The boy, Charlie, is now able to express his basic needs.
“He’s also learned safety skills like being able to ‘stop’ when someone asks him to,” Lamb said in a statement provided by Autism Speaks. “ABA was also successful in helping Charlie through his fear of the doctor and dentist. We don’t have to put him under anesthesia for dental exams/interventions anymore, which is incredible.”
Similar glowing recommendations from parents abound. Last summer, a group of Indiana parents staged a protest after being alerted by their kids’ therapy centers that the state wanted to cut reimbursement rates. They gathered outside the governor’s mansion, holding signs that said, “ABA is the way” and, “They wouldn’t be who they are today without ABA.”
In Virginia, then-Delegate Bob Thomas kicked off a 2019 press conference announcing a push to expand access to autism therapy by asking the grandson of a local advocate to step to the dais.
“Mark is a great example of why we are here today,” Thomas said, explaining that the child had once been unable to speak. “Thanks to the services and the resources Mark had access to, he’s now able to stand here in front of a roomful of media, media cameras and lead us in the Pledge of Allegiance.”
In response to a reporter’s question about what was at stake, a mother of three autistic boys stepped to the mic: “If it weren’t for the behavior therapy that we receive, we would not be able to go out in public like this today.”
Add to displays like these effusive testimonials on ABA center websites, memoirs penned by parents who credit ABA with their children’s miraculous recoveries and whispered confessions from caregivers that the therapist’s arrival gives them a much-needed break from kids who require constant supervision.
Research has begun to probe the disconnect between parents’ and children’s perceptions. The 2018 Advances in Autism study, for example, predicted that nearly half of autistic children exposed to ABA will meet the threshold for a PTSD diagnosis within four weeks, while caregivers’ satisfaction will rise as the treatment goes on.
Still, the study noted, 9% of caregivers surveyed discontinued the therapy because they didn’t see enough progress or saw negative changes. Overall, “caregiver satisfaction was generally reported within the neutral range. The longer a child was exposed to ABA, the more likely a caregiver was to rate the intervention as effective for improving overall functioning.”
Have you seen Mr. Potato Head?
Denise’s son Logan was 27 months old when a neurologist at the prestigious Boston Children’s Hospital diagnosed him with autism. He was smart and carefree but very rambunctious, more likely to throw toys than play with them. He never spoke words but used his voice to stim. (To protect Logan’s privacy, he and his mother have been given pseudonyms. The family lives in western Massachusetts.)
Home to numerous elite research universities — including Harvard, where behaviorist B.F. Skinner planted ABA’s conceptual roots — Massachusetts is considered a great place for autistic children. It was one of the first to mandate insurance coverage for autism services and now contracts with 22 companies to provide intensive early interventions. ABA dominates the offerings.
Eager to get her son as much help as possible, Denise got him on wait lists for two treatments: ABA and a lesser-known approach called Floor Time. Within two weeks, an ABA therapist was spending 14 hours a week with Logan.
For a while, Denise says, things went fine. But when COVID-19 forced the therapy online, Logan balked.
“The idea that he was hiding in the closet because I was turning on the computer for ABA was just like a total alarm going off,” she says.
Denise told the therapist the discrete trials didn’t seem like a good fit, fears that were compounded when in-person services started back up. At her first visit, the therapist invited Logan to jump on a trampoline with her. She pointed a finger skyward and said, “Up, up, up.” Pointing his own finger, a delighted Logan started shouting the word with her. Saying words out loud was new for him.
The victory was short-lived. The therapist moved on, asking Logan to put his hands in water. Still excited, he kept pointing and chanting, “Up, up, up” instead. The response was gentle but devastating: The therapist folded his finger down and moved his hands where she wanted them. The boy shut down.
“To see the joy disappear from his face — all of a sudden he’s no longer a willing participant,” Denise recalls. “There was no abuse or anything, but she made him comply.”
Denise canceled Logan’s ABA. Meanwhile, his name had come up to the top of the Floor Time wait list. Floor Time uses play-based activities that the child chooses. The aim is to make interactions increasingly complex.
During the first session, Logan picked up a Mr. Potato Head and threw it. Denise watched with bated breath, anticipating negative reinforcement. But the new therapist started throwing toys, too. And then wandered the room picking up toys and asking in a silly voice if they had seen Mr. Potato Head.
“All of a sudden, [Logan] is picking up a toy and perfectly imitating her intonation — without words, but her tone perfectly,” says Denise. Next, he held toys in front of his mouth and said words for them. Soon, Logan was a chatterbox, talking about the dream he had the night before, ways to defeat bad guys, becoming a superhero — everything.
Insurance codes and new markets to mine
As recently as the year 2000, insurance coverage was not required for autism therapies, which researchers estimate cost from $10,000 to $100,000 per year. After fierce lobbying, by 2017 advocates succeeded in pushing laws requiring reimbursement in 46 states. As this sea change was taking place, ABA therapists were among the few people with formal credentials who could step into jobs created to help families access newly covered services.
This meant that ABA practitioners were often the ones who created insurance billing codes, referral networks and other systems, making them de facto gatekeepers. As a result, though many states require coverage for other types of therapy, getting care other than ABA can be incredibly difficult. Parents who get referrals for speech and occupational therapists, or for augmentative and assistive communication technology for their nonverbal children, often find that the only available providers typically offer ABA.
Revel Weber has firsthand experience with this. A clinical social worker and the autistic parent of four children, one of them autistic and two with ADHD, several years ago she was asked to create a program to serve autistic children belonging to the White Earth Nation in northern Minnesota. As part of her research into treatments that would both benefit tribal families and qualify for public funding, Weber took some online ABA training courses.
She quickly decided it wasn’t appropriate for White Earth children. In addition to being uncomfortable with the focus on compliance, Weber, who is not American Indian, believed ABA could play negatively into historical trauma associated with attempts to assimilate Native children.
Like many states, Minnesota requires insurers to pay for a number of autism therapies, but as Weber explored alternatives to ABA, she ran into a maze of red tape. In their rush to provide the greatest access to services, the government created Medicaid reimbursement codes — the backbone of health care billing — that reflected the most available treatments. The majority were ABA. Thirty-seven years after Lovaas’ bombshell study, there are numerous ways to become an ABA therapist, ranging from full-fledged degrees to online courses. But there are far fewer providers of other kinds of treatments. Those ABA therapies are now locked into the codes, meaning billing for anything else can be difficult.
The ABA sector’s strategies for making its services widely available were smart, says Jeffrey Guenzel, head of the International Council on Development and Learning, which provides Floor Time training. But it has made it challenging for other therapies to become established.
The intervention’s rapid spread has also resulted in uneven quality, even supporters like Shih, of Autism Speaks, say. Some practitioners hold credentials that may require an advanced degree and long experience, while others — typically identified as technicians — may have taken only a few hours of virtual training.
Venture capitalists are up front in saying the increase in autism diagnoses and continued unmet demand suggest the sector is poised for explosive growth. In a market overview, one investment company asserted that there are about 1 million autistic children in the United States. In 2020, the analysis said, ABA programs generated $1.4 billion — a figure expected to grow to $2.45 billion by 2025. And there are new markets to mine.
“ABA treatment is widely recognized as the most effective method for treating [autism], but its evidence-based treatment methods are applicable beyond [autism] alone,” the brief asserts. “Mental health issues in schools and the provision of more providers will ultimately expand ABA recognition beyond [autism] exclusively.” Other areas of opportunity, the investment bankers’ materials say, include ADHD, Obsessive-Compulsive Disorder, Panic Disorder, Oppositional Defiant Disorder and PTSD.
The one and only option
For the first few years after earning a degree in special education, Ryan Haenze, himself autistic, taught in Twin Cities school districts. His training was to let students’ interests steer his instruction, but this wasn’t what his higher-ups wanted. They wanted behavior management, he says — specifically, compliance.
The kind of instruction he favored because of his autism — sensory accommodations, interactive projects and movement breaks for the kids — earned him bad evaluations. “I had administrators saying, ‘What you are doing is not best practice. You need to physically put these kids into chairs, do hand-over-hand,’ ” says Haenze, meaning moving the child’s hand with his own. “It needed to be those specific, very structured methods.”
Haenze repeatedly pointed out that those strategies often lead to explosive behavior. Once, he said, he watched helplessly as one of his third graders was removed from school in handcuffs.
At many schools like Haenze’s, administrators adopt ABA principles because they are viewed as best practices. But other places take a more formal approach. For example, Boston Public Schools now offers ABA in every school. Between 2011 and 2021, The Nation reported, the number of behaviorists in the district doubled. Families with autistic kids in Cambridge Public Schools are routinely placed in ABA-aligned classrooms.
Many communities have privately operated ABA schools that students attend full time at district expense. Haenze says most of his students received therapy at ABA centers as toddlers and preschoolers. In kindergarten, they began spending half their day at school and the rest at an ABA center — a common arrangement.
However, the U.S. Department of Education’s Office of Special Education and Rehabilitative Services has warned schools not to let ABA crowd out other services that are supposed to be considered for students’ Individualized Education Programs. Specifically, the department said it had received reports that a growing number of children were not being evaluated by the range of professionals who typically determine what the appropriate — and under a child’s IEP, legally mandated — services are.
“Some [special education] programs may be including applied behavioral analysis (ABA) therapists exclusively without including, or considering input from, speech language pathologists and other professionals who provide different types of specific therapies that may be appropriate,” the department warned. “We recognize that ABA therapy is just one methodology used to address the needs of children with [autism] and remind states and local programs to ensure that decisions regarding services are made based on the unique needs of each individual child.”
Communication support is one accommodation that has become increasingly scarce as ABA’s strategies for teaching children to be verbal have spread, says Zoe Gross, director of advocacy at the Autistic Self Advocacy Network. Because many people believe spoken words are superior, special educators often aren’t trained in the alternative technologies, she says.
For Haenze, being an autistic teacher unable to convince his co-workers he had useful insight was maddening, he says. Receiving poor evaluations from supervisors unwilling to consider that his ideas might make classrooms calmer and students more engaged was demoralizing. Worse, he says, was neurotypical teachers’ misunderstanding of their students’ capacity for self-expression — and, by extension, their intellect.
Midway through his sixth year, Haenze quit teaching and went to work for the Minnesota Disability Law Center as an advocate.
‘I don’t ever want them to feel shame’
Given the prevalence of ABA, it is difficult even for parents who don’t want to engage with the treatment to avoid it entirely. Denise says that for a long time, she was asked at Logan’s pediatrician check-ups whether he was getting the therapy. It made her nervous to say no, over and over again, and know that answer is being entered into an official record. Eventually, though, it was so clear the boy was thriving that the conversations stopped.
Elizabeth, too, rejected offers of ABA interventions many times, simply saying her family doesn’t think it is a good fit for Lily. She believes she got away with turning down services because her daughter doesn’t engage in many behaviors that schools typically try to eliminate.
Weber has gone a step further — choosing, based on her experience as both a therapist and an advocate for her children, not to have her autistic son diagnosed or evaluated for special education, where she would have to fight to turn down ABA-related services.
“I am trying to avoid that,” she says, choosing instead to work with the boy and his two neurodivergent brothers herself, at home. “I don’t ever want them to feel shame. I always want to instill pride in who they are.”
This story was produced by The 74 and reviewed and distributed by Stacker Media.
